The case presented is a patient in whom an MRI examination under weight-bearing conditions was able to establish a diagnosis that could not be demonstrated by a conventional supine MRI.
History: The presented 77-year-old patient complained of load-dependent lumboischialgia for more than one year. Nine months prior to the Upright MRI examination, a synovial cyst of the left lesser vertebral joint L4/L5, which was considered causative for the complaints, had been removed. The back pain and right leg pain have improved. The pain in the left leg along the L5 – dermatome was improved for only three months. In case of persistent complaints, a Coflex implant has been inserted between L4 and L5 one month before the Upright MRI examination to achieve stabilization of the affected segment. Postoperative complaints were identical to the preoperative situation. A supine examination showed ubiquitous degenerative changes without higher grade spinal or neuroforaminal narrowing, as was the case preoperatively.
Upright kinetic-positional MRI was then performed to rule out functional instability.





A-B: Sagittal standard exposures in supine position
C-D: Sagittal functional images
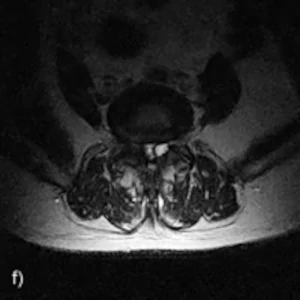
E-F: Axial exposures in sitting position under natural weight load at L4-L5 level.
The examination:
Standard MRI examination in the supine position: Conventional supine MRI examination confirms exclusion of higher grade neuroforaminal or spinal stenosis in Z.n. Coflex implantation L4/L5.
Upright MRI functional examination under natural weight bearing: Under weight bearing, there is a high degree of spinal tightness L4/L5 caused by a degenerative anterolisthesis from L4 to L5 of 7mm in severe bilateral hypertrophic spondylarthrosis. Ventral displacement does not change in any position under weight bearing. Spinal tightness is accentuated by bilateral synovial cysts bulging intraspinally from the small vertebral joints L4/L5 bilaterally. The cysts have a diameter of 11mm on the left and 6mm on the right side. In the reclination position, as in the standing position, there is an accentuation of the spinal constriction.
The findings on the Upright MRI: The examination shows a high-grade spinal tightness with accentuation in reclination and in stance with unstable, degenerative anterolisthesis L4 on L5 in severe hypertrophic spondylarthrosis and after intraspinal reaching synovial cysts, left accentuated.
The presented case impressively underlines the dynamic component and the various factors that can lead to spinal stenosis. Conventional MRI in the supine position alone cannot show these components.