The 57-year-old patient presented here complains of chronic lumbar syndrome for one year in condition after lumbosacral fusion surgery (2000) with persistent lumbaralgias and pseudo-radicular lumboischialgias.
Left-sided accentuated radiation into the laterodorsal leg region up to the foot area with stress- and position-dependent accentuated symptoms. During walking with additional gait instability and limitation of walking distance.
The presentation was made for clarification of the lumbar spine under natural weight bearing as well as in functional positions in case of clinical suspicion of lumbar sliding instability.
A 5-month-old out-of-hospital preoperative conventional supine MRI examination did not yield a definitive diagnosis.
Upright MRI examinations were performed under natural weight bearing in a neutral upright sitting position, as well as in inclination in sitting and in reclination in standing.
In the five-month-old supine examination available for comparison (Fig. a), there was no clear explanation for the patient’s existing complaints.
Only the performed upright MRI provided information about the load- and position-dependent symptoms:
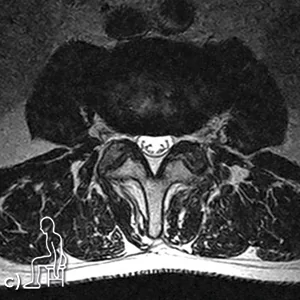
The leading symptom is a function-dependent absolute spinal canal stenosis in segment L3/L4, in the reclination position in the standing position (Fig. d,e) with pincer-shaped segmental constriction of the cauda fibers.
This is caused by a broad-based disc protrusion clearly extending into the neuroforamen as well as thickened lig. flava and a prominent posterior epidural lipomatosis. The remaining a.p. diameter of the spinal canal is still about 3-4mm in standing position.




Upright MRI examination under natural weight bearing and in various functional positions provided a definitive diagnosis explaining the patient’s symptoms of discomfort.
a) The supine examination does not show a clear explanation for the patient’s existing complaints.
b) T2-sagittal in sitting position;
c) T2-axial in sitting position at the level of L3/L4;
d) T2-sagittal in pain position in reclination in standing position;
e) T2-axial in pain position in reclination in standing position at the level of L3/L4.