A conventional MRI of the cervical spine performed in the supine position did not provide a clear diagnosis for the complaints. Upright MRI was then performed to clarify the cervical spine under natural weight-bearing and in functional positions (anteflexion and retroflexion).
Presented here is a 39-year-old female patient with a known, conservatively treated cervical disc herniation in the C6/C7 segment.
The patient complains of chronic cervical syndrome with recurrent neck pain, vertigo attacks with vomiting, and pseudoradicular cervicobrachialgia radiating to the right, with a marked position-dependent increase in complaints in retroflexion (extension), as well as a marked limitation of movement in the head and neck region.
An external MRI of the cervical spine, performed conventionally in the supine position, did not provide a clear diagnosis for the complaints. The patient was then presented for an Upright MRI to clarify the cervical spine under natural weight-bearing and in functional positions (anteflexion and retroflexion).



a) External exposure sagittal T2 in supine position
b) Sagittal T2, neutral position in sitting position
c) Sagittal T2, inclination in sitting position
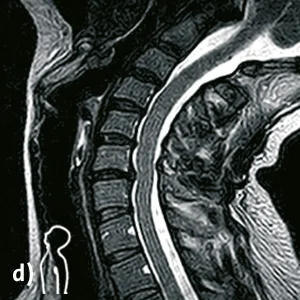
d) Sagittal T2, reclination in sitting position
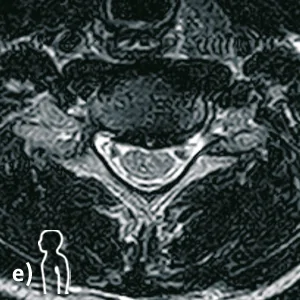
e) Transversal T2, neutral position in sitting position at height C6/C7
Diagnosis / Findings:
In the neutral position in the sitting position, there is a clear extension malposition of the middle cervical spine with kyphosis tendency as well as a persistent cervical steep position with limited mobility of the upper and middle cervical spine in anteflexion.
In the segment C6/C7 a broad dorsal disc prolapse with myelon contact with regression tendency in anteflexion and accentuation in retroflexion is seen in neutral position in sitting. In the retroflexion position, a function-dependent spinal canal stenosis with narrowing of the cervical myelon to an ap diameter of approximately 8mm at the level of the disc prolapse is seen.
In the segment C5/C6, a disc protrusion is seen in the neutral position, which clearly recedes in the anteflexion posture and clearly accentuates to a functional myelon contact in the reclination posture (overall borderline to a dorsomedian disc prolapse).
The segments C4/C5 and C5/C6 show angular instabilities with an increased opening of the disc spaces in reclination posture of more than 10 degrees compared to the inclination posture.
In the segments C3/C4 and C4/C5, shallow dorsal disc protrusions are seen in the reclination posture.
Upright MRI functional images provided a definitive diagnosis that could not be made by conventional supine MRI.