The 44-year-old female patient presented here has been complaining of complaints in the area of the cervical spine with radiation to the head and face for about a year. The complaints existed mainly in an upright position, especially strong when leaning backwards. The clinical examination revealed a suspected nerve root compression at C7.
A conventional magnetic resonance imaging examination performed in the supine position revealed a protrusion (approximately 3mm) at C5/C6 without significant narrowing of the spinal canal and without affecting the nerve roots.
Due to the persistent complaints, an upright MRI was performed, under the natural weight bearing of the cervical spine with additional functional images in inclination and reclination.
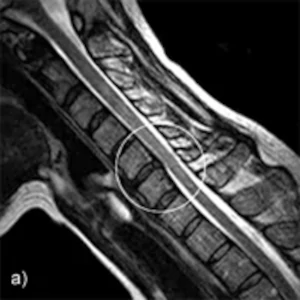

A-B: Sagittal images in the sitting position: Inclination and reclination
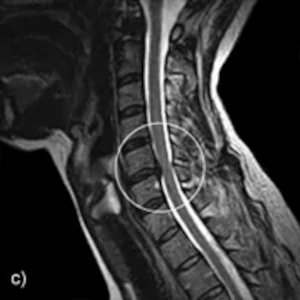
C: Sagittal image in sitting position in neutral posture
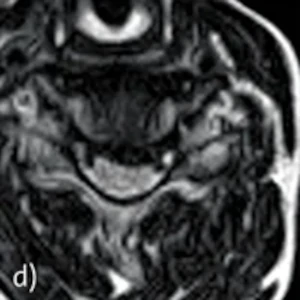
D: Axial exposure in sitting position in neutral posture
Findings: Upright MRI examination was performed in the sitting position, upright and under natural weight bearing. The images in neutral position show a median / mediolateral to intraforaminal left radiating disc prolapse with compression of the myelon and also compression and displacement of the C7 nerve root left interspinously. The disc overhangs the vertebral body level dorsally by 5mm. This reduces the ventrodorsal diameter of the central portions of the spinal canal to 6mm.
Functional images showed a decrease in the size of the disc prolapse in the inclination position with an increase in the width of the central portions of the spinal canal to 8mm.
The functional images in reclination showed a marked increase in the size of the disc findings, especially in craniocaudal extension with marked protrusion of the posterior longitudinal ligament. In addition, a prominence of the ligamenta flava was seen, resulting in a central narrowing of the spinal canal to 4.5 mm.
Functional examination in the Upright MRI, upright under natural weight bearing, clearly diagnosed the cause of the complaints. The clinical suspicion of a nerve root compression could be confirmed, additionally a position-dependent compression of the myelon could be proven.