The patient presented here suffered a myelon contusion during a fall down stairs in 1999. The fall was immediately followed by paraplegia with complete flaccid paresis of both arms and legs. A rehabilitation treatment resulted in incomplete restitution, with spastic tetraparesis still present on the right side more than on the left.
.


A-B: Sagittal images in the sitting position: Neutral position and reclination
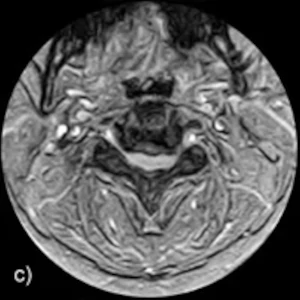
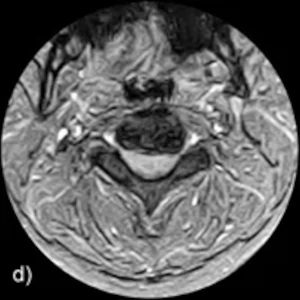
C-D: Axial images in sitting position at height C2-C3: Neutral position and reclination
Findings: Functional radiographs under natural weight bearing demonstrate instability at C2/C3. In the neutral position, there is a high-grade spinal narrowing at the level of the disc C2/C3. The spinal canal is highly, pincer-like narrowed by retrospondylosis, disc protrusion and a dorsal bone spur. The myelon is compressed and significantly thinned. In the inclination position, the disc protrusion at C2/C3 is markedly flattened. Also, the circumscribed protrusion from the dorsal side is no longer present, so that the spinal canal now appears considerably wider with decreased compression of the myelon. In reclination, the spinal narrowing is increasing.
Diagnosis: Upright™ MRI of the cervical spine reveals a high-grade narrowing of the spinal canal with significant compression of the myelon in the neutral position at C2-C3. This is due in part to protrusion of the disc, possibly also aided by infolding of the posterior longitudinal ligament and detachment of the ligamentum flavum dorsal. In the inclination position there is a clear widening of the spinal canal, probably due to a flattening of the disc protrusion at C2-C3 and due to the fact that the ligamentum flavum now lies dorsally.