The 60-year-old patient presented here complains of a chronic recurrent lumbar syndrome that has been accentuated for 2 years with pseudoradicular lumboischialgia with bilateral, load- and position-dependent radiation into the legs as well as restriction of walking distance.
A preliminary examination in the supine position did not yield a definite diagnosis. An Upright MRI was performed to clarify a dynamic spinal stenosis.
Upright MRI examination was performed under natural weight bearing in a neutral upright sitting position and in flexion in sitting and extension in standing.
Five-month-old off-site MRI images of a conventional supine examination were available for comparison.





a) Sagittal T2 in supine position
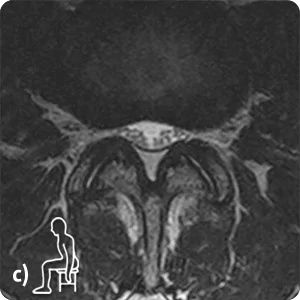
b) Sagittal T2 in sitting position, c) Axial T2 in sitting position at L3/L4, d) Axial T2 in sitting position at L4/L5
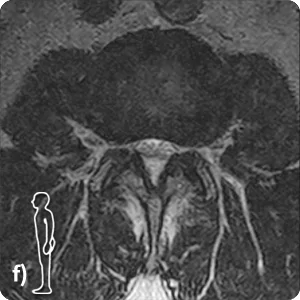
e) Sagittal T2 in standing position, f) Axial T2 in standing position at L3/L4, g) Axial T2 in standing position at L4/L5.
Diagnosis:
In the five-month-old supine examination available for comparison, no clear explanation for the patient’s existing complaints was found. Only the performed Upright MRI provided information about the position- and load-dependent symptoms:
In the segment L4/L5 a function-dependent, absolute spinal canal stenosis with pincer-shaped constriction of the cauda fibers presents in extension posture in standing position.
In the segment L3/L4 a function-dependent, relative spinal canal stenosis with constriction of the cauda fibers as well as a function-dependent pseudospondylolisthesis with functional anterolisthesis of L3 (ventral displacement of 3-4 mm / grade 1 according to Meyerding) with inconspicuous posterior edge alignement in the supine and sitting position is shown in the extension posture in the standing position.
The neuroforamina in segments L3 to S1 are significantly constricted on both sides under natural weight bearing in sitting, but especially in extension posture in standing.